Introduction
Hair loss due to disease, scarring and in particular, androgenetic alopecia, has troubled members of the human race since the dawn of history. A prescription for restoring hair is included in the Ebers papyrus of ancient Egypt which has been dated at 1800 B.C. (1)

The first attempts at surgical restoration of hair loss were recorded by Dieffenbach in 1822. In his inaugural thesis at Wurzgurg, he described animal investigations in all and auto-transplantation of hair, skin, and feathers. (2) Autografts of the hair-bearing scalp using flaps and large free grafts have been in use since at least 1893. (3) A Japanese surgeon Sasagawa reported hair follicle transplantation as early as 1930 (4) and in 1939 Okuda, a Japanese Dermatologist, described the correction of alopecia of the scalp, eyebrow and mustache areas using small cylindrical punches to remove the donor tissue and slightly smaller ones for the recipient area. (5)
Tamura transplanted single hairs to the pubic area in 1943 (6) and Fujita in 1953 reported the use of this technique for a wide variety of defects. (7) No Japanese author mentioned the use of this technique for the correction of male pattern baldness and because of wartime conditions, the work went unrecognized outside of Japan.
Orentreich, a New York dermatologist studied the donor or recipient dominance of various alopecia conditions and reported this work in 1959 (8). He noted that donor dominance was observed in all cases of male pattern alopecia and was able to refute the prevailing theories that male baldness was a result of poor blood supply to selected regions of the scalp. His paper captured the attention of the public and many other dermatologists were trained by him. It can be rightfully claimed that modern hair restoration techniques date from this time.
Since then there has been a wide variety of surgical procedures described (9) but for the sake of brevity, only those still in frequent usage will be discussed in this review.
Hair Restoration Techniques
There are three broad categories of surgical hair restoration procedures These may be summarized as follows-
- surgical excision, (alopecia reduction)
- scalp flaps (advancement flaps, rotation flaps, and free flaps )
- free autografts of hairy scalp from the well haired to the bald area (these grafts may be from a diameter of about 5mm down to a single hair follicle.)
All three categories of operation are still performed at the end of the 1990s but the most generally accepted are the autograft techniques known as “micrografting”, “mini grafting” and “follicular transplantation”.
1. Alopecia Reduction Surgery
This procedure was introduced in the mid-1970s in Canada (10) and due to its simplicity and speed of results, gained rapid acceptance (11, 12). Within 1-2 years the operation was being performed in enormous numbers worldwide
The basic philosophy of removing part of the balding region and undermining so as to close without undue tension was very appealing. Many ingenious designs were introduced and their various merits argued loud and long at Hair Restoration meetings.
Unfortunately, there are other factors operating which negate the beneficial effects of this procedure and within a few years, the first warnings were being given (13). The problems were caused by the tendency of the balding area to stretch again if even the slightest tension was present and more importantly, by the natural progression of the androgenetic balding process with time. Worse still, the stresses of the surgical procedure itself were accused of accelerating the progression of the balding. The mechanism of this can only be speculated, but the end result was often the rapid recurrence of baldness, visible scarring and patient disappointment within a few years.
In recent years many procedures and devices have been proposed to lessen the effects of “stretch back” and other associated problems. These include the Frechet Extender, the Seery periosteal anchor flap, the Unger Prolonged A.T.E, and the Nordstrom Silastic suture, (14, 15, 16, 17 18)
Marzola (19) tackled the problem of the unsightly central scar from a different approach by electing not to fully close the posterior bald area and by using an “M” shaped incision.
By the end of the 20th century, the use of alopecia reduction had declined markedly and most surgeons were using these techniques only for highly selected cases, if at all. This is probably an over-reaction and it is likely that the technique will be revived in future years. With the benefit of improved techniques, more caution used in case selection and greater attention to surgical detail during the operation, more satisfactory results may be expected.
2. Flap Surgery
Scalp flaps for reconstructive surgery of the scalp had been in use since the 1890s (3). Short hair-bearing pedicle flaps to disguise scalp scars were first described by Passot in 1919 and again by Lamont in 1957 but made very little impression on the world medical community (20, 21) Scalp flap surgery received an enormous boost when Argentinean surgeon Jose Juri, who used long Temporo-Parieto-Occipital flaps, described his twice-delayed methods at plastic surgery meetings in 1972 and 1975 and published his results later that year (22)
The technique was quickly adopted by courageous but inexperienced surgeons worldwide with varying results. Tip necrosis wound breakdown and sloughing of the entire flap was not uncommon. The technique has a considerable “learning curve” and was unforgiving if short cuts were taken.
In 1980, Kitaro Ohmori pioneered microsurgically anastomosed free flaps, a lengthy and technically difficult procedure with a varying degree of success. (24) Gradually, many surgeons abandoned hair surgery altogether or switched back to the safer, shorter flaps and a number of inventive variations were introduced in the following years by Stough, Nataf, Dardour, Bouhanna, Frechet, Nordstrom and others (25).
The introduction of tissue expanders in the 1980s made the flap techniques safer by increasing the area of available donor scalp and enabling tension-free closure of the wounds. In spite of these advances, the residual scars in both donor and recipient sites often left a cosmetic problem for which no adequate solution existed and the operation gradually slipped in popularity with both patients and surgeons. Newer techniques for free grafting were developed and by the end of the 20th-century scalp flap surgery had been abandoned by all except a few highly experienced surgeons who specialized in this technique (26).
3. Scalp Autograft Surgery
Free scalp autografts are very reliable providing they are carefully handled and recipient areas can provide enough oxygen and other nutrients to sustain life and growth. Once the boundaries are pushed beyond certain parameters problems begin to occur. The difficulty is that there are as yet, no hard and fast rules for graft survival. Grafts up to 5 mm in diameter will produce 100% growth in certain situations while grafts of less than 1 mm will fail if trimmed improperly or packed too closely together in some scalps.
It is important to get rid of excess dermal components before attempting to insert grafts close together in large numbers of up to 50 grafts per square centimeter yet single-hair grafts will fail if trimmed excessively of sebaceous components and stem cells for future growth.
For 25 years variations on the original Orentreich technique remained in vogue and sessions of from 40-100 x 4.0 mm grafts were transplanted from the donor site to slightly smaller recipient sites in the bald area. Smaller 2.0 mm grafts were used by some surgeons in the 1970’s but received no publicity at the time. Sessions of up to 240 grafts created by quartering 60 x 4 mm grafts were being performed by Wayne Bradshaw of Australia in the early 1980s and extended to over 400 later. (27, 28)
Dr. Carlos Uebel of Brazil (29) appears to have been the first to perform and speak on larger sessions of up to 1000 small grafts from around 1983 but the technique did not receive widespread publicity until the Moser Group in Austria introduced their paper and videotape on the procedure at a meeting in Rio de Janeiro in 1992. (30)
Dr. William Rassman of California pushed the boundaries of the procedure out to over 3600 grafts by 1994 (31 ) and started bringing large numbers of patients, in various stages of completion to Hair Restoration meetings. From that time onwards the technique became widely accepted and underwent continuous refinement. ( 32, 33)
The use of microscopes for the dissection of grafts was introduced by Dr. Bob Limmer in 1987 (34) and was slow to gain acceptance because it tripled the time required for graft preparation Growing disquiet concerning the poor growth which sometimes resulted from the dense packing of mini grafts (35) led to its gradual acceptance however and, championed by Seager, Bernstein, Norwood, and others, the use of this technique appears to be in the ascendancy as we enter the new millennium.
Follicular Unit Transplantation Techniques
In this increasingly popular procedure, large numbers of hairs are harvested, with the aid of a 10 power binocular microscopes, from a strip of excised full-thickness scalp. These naturally occurring follicular clusters each containing 1-4 hairs are then planted into needle holes in the balding area. This is a refinement of an earlier technique known as “mini grafting” in which the follicular clusters and some surrounding skin was planted into slits cut in the scalp with a small scalpel blade.
Large numbers of hairs can be inserted at a single procedure with either technique providing certain safeguards are met and quite extraordinary results may be seen within 4-5 months of operation. The advantage of follicular unit grafting is that a greater hair density can be obtained and figures of up to 61 hairs per square cm. in a single procedure have been claimed. (36 )
The technique has the disadvantage of being more time consuming, taking between two and three times the number of work hours to dissect and insert the same number of hairs. This has a considerable economic impact on the patient. Proponents defend this by claiming that in good hands the number of donor hairs damaged during the procedure is at least 20 % less than with non-microscopic methods of dissection. (37) However, it has been suggested that follicular trans-section and bulb amputation are not as important as once thought and considerable hair regeneration will occur if the follicular stem cells have been preserved. (38) These points and the future direction of free grafting remain highly debatable points as we enter the new millennium.
Variations in Techniques
There is a wide variation in the technique used by the various surgeons performing hair transplantation. We need not be concerned about the finer points of the procedure in this review as many excellent descriptions are available in print and video format. (38, 39) There are numerous minor variations such as whether the surface epithelium should be removed or not, or whether a razor blade or scalpel is used for the dissection. Whether sutures or staples are employed may be a matter of convenience for the surgeon or comfort for the patient but have little effect on the cosmetic result. These are points of individual preference and there are broader issues that must be addressed.
I have listed these as follows:
- Graft Numbers and Graft Density
- Tumescent Anaesthesia
- Single Blade Vs Multi-blade knife.
- Role of the Stereoscopic Microscope
- The Recipient Site
- Role of the Surgical Laser
1. Graft Numbers and Graft Density
For an average Type, 6 bald scalp of dimensions says 12 cm. x 20 cm. there is a bald area of about 200 sq. cm. Even at a density of only 40 hairs per sq. cm. this will require 8000 hairs. This can be achieved with the use of 3500 follicular unit grafts or 2000 small mini grafts if distributed evenly throughout. Most surgeons prefer to place in excess of 60 hairs per cm sq. along the frontal hair zone and this can be achieved in a single session by some skillful surgical teams with very suitable patients. (36)
One cannot safely place large numbers of bulky mini grafts containing excess skin elements into Slits or holes at a density of much greater than 16 per sq. cm in a single session although this would yield a result in excess of 60 hairs per sq. cm if all grew successfully. To achieve density the grafts must be more carefully prepared to discard redundant tissue and isolate the pilosebaceous units. If single or double hair groupings are required it is best if these are selected from naturally occurring groupings rather than artificially creating small units by cutting down larger ones. (32)
The placing of grafts very close together has been termed “dense packing” (40)and it is this aspect which has to attract the most criticism. Cases presented at meetings have shown how successful the technique can be with ideal patients, but opponents have described instances where hair growth is much less than optimal, and even cases where, allegedly, “no growth” has occurred. (41) Drs. Rassman and Bernstein have agreed that such cases have been seen in their practice but call them “delayed growth”, insisting that significant growth can occur after 12 months in some cases. (42) This point awaits further clarification.
2. Tumescent Anaesthesia
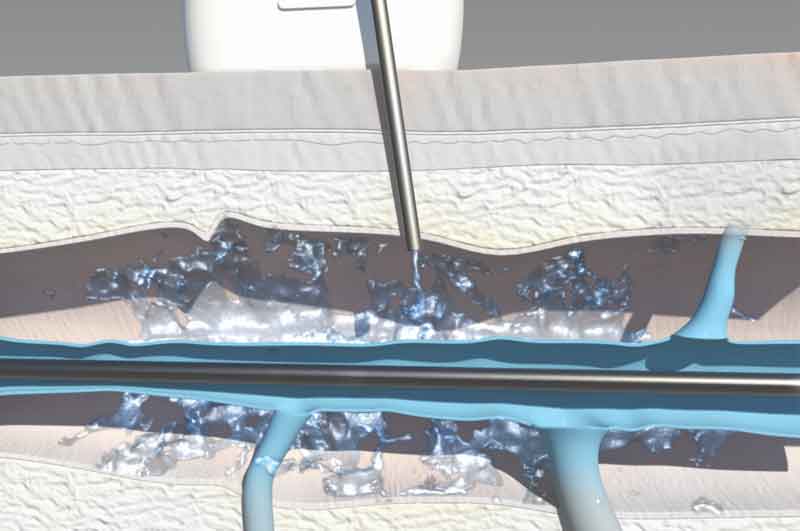
First introduced as an aid to liposuction, (43) this technique, in a modified form, has been embraced by hair transplant surgeons. (44.) The aim is to distribute very dilute solutions of local anesthetic and vasoconstrictor evenly throughout the donor and recipient sites. At the donor area, this results in a bloodless, firm cutting surface and for the recipient site, the dermis is thickened so that one is less likely to strike the larger blood vessels which lie just above the galea.
Operative blood loss may be greatly reduced with this technique with beneficial effects for patients and surgeons. The operation proceeds much more smoothly without the operative site obscured by blood and recently inserted rafts continually “popping”. For the patient, there is the advantage of less total blood-loss and decreased postoperative swelling and bruising around the forehead and eyelids.
Epinephrine (adrenaline) is the most commonly used vasoconstrictor and is generally added to the anesthetic agent in a concentration of 1:100,000. In Australia, New Zealand and some European countries the excellent synthetic drug 8-ornithine vasopressin (P.O.R-8, Sandoz) is available. (45) Unfortunately, vasoconstriction is not always fully adequate with any currently available technique or vasoconstrictor. Vigorous and persistent bleeding is frequently encountered with young men who are very active physically and it is known that preoperative anti-inflammatory agents can have a profound negative effect on the speed of coagulation. Alcohol, aspirin and vitamin E are known offenders and it is possible that other agents such as marihuana may be detrimental to coagulation. Some surgeons like to infiltrate troublesome regions with small amounts of anesthetic containing adrenaline 1: 25,000. (46) Significant changes in pulse rate or regularity are surprisingly rare in these cases.
3. Single Blade Vs Multi-blade Knife
In a recent survey, 73% of respondents were using the multi-blade knife. (47) On the other hand, it is interesting that most of those using the stereoscopic microscopes now use a single blade (48) The argument is that follicular damage is proportional to the length of the unmonitored incision line. For a single 15 cm strip, there will be approximately 30 cm of cut which is all made under visual control. With a multi-blade knife, it is claimed that only the top blade can be closely supervised and the other 2 – 9 blades cut blindly through the donor tissues.
While there is undoubtedly a measure of truth in this argument, Dr. James Arnold of San Jose, California, has shown us ways to minimize the potential damage caused by the multiple parallel scalpel blades. (49,50) This includes thorough infiltration of the superficial donor tissues with saline and vasoconstrictor, use of the Persona Plus #10 blade for extreme sharpness, the slow movement of the cutting knife using the fingers and wrist only and frequent checking of the several strips for change of direction of the emergent hairs. Using these techniques and a little practice, the strip is almost perfect every time.
The thin strips are easily dissected on a wooden tongue depressor blade or on a trans-illuminated plate( 51). The donor skin in some individuals is very soft and difficult to cut accurately. This has been termed “mushy dermis” and the multi-blade knife should not be used with these individuals. (52) Dissection of a single broad strip into thin cross-slices or “slivers”, is extremely difficult as it has no remaining turgor. Unless great care is taken, any advantages achieved by the single blade strip excision may be lost in the slicing process. This is where microscopic control is so useful, although frustratingly slow.
Semi-automatic dissection devices constructed from an array of closely spaced blades have been available for several years. The merits and demerits of these devices are still being hotly debated. (53, 54)
4. Role of Stereoscopic Microscopes
The use of stereoscopic dissecting microscopes was pioneered by Dr. Robert Limmer of San Antonio, Texas in 1987 (34) but has been slow to gain acceptance. Apart from the sheer technical difficulty of graft preparation at high magnification, there is considerable disruption to existing staff work-practices. The number of work-hours per operation is more than doubled compared with regular mega-session work. This means long hours of work or the employment of more assistants. Either way, there is a considerable disruption to the equilibrium of any Hair Replacement Clinic making the change and the possible advantages must be weighed against the disadvantages. (55)
Whether a general change to stereoscopes is justified at this time is still being debated and many Clinics obtain outstanding results with naked-eye dissection or with the use of low power binocular loupes. Careful inspection reveals that there is certainly the potential for less damage to follicular units with the use of higher power magnification but it is all very much dependent on the skill of the Assistants. It has been stated that when using the microscope 20% less donor strip is required to obtain the same number of well-trimmed follicular units. (32) If donor tissue is in short supply, stereoscopic microscope dissection would certainly appear to be the method of choice.
It is worth remembering that although lip service is paid to the adage that “every scalp hair is precious” there is, in fact, an awful lot of them. Surveys show that only 23 % of men have so much baldness by the age of 70 years that there is likely to be a severe shortage of donor follicles if they chose to push the technique to the limit (55) Experience has shown that only a tiny percentage of men present for transplants or continue to have transplant sessions into their 7th decade, even if adequate follicles are available. Hair graying and a general decrease in motivation seems to lessen the obsession for more hair that so dominated the earlier years of these individuals.
The change to microscopic dissection might be forced by factors in addition to donor supply. If, for instance, it could be shown that there was faster hair growth or less hair “crinkle” after microscopic preparation of the follicular units, this would potentially affect all patients and not just the small percentage for whom the future supply is a critical factor.
5. The Recipient Site
Once the spacing in mega sessions becomes closer than about 16 per sq. cm. it is no longer advisable to make all the recipient sites with a No 11 or 15c blade. The slits or holes must be tailored much more precisely to the size of graft being used and most operators have moved to the use of 16 and 18 gauge Nokor needles. An alternative system is provided by A-Z Instrument’s “Lightning Knife”. The handle takes SP 91 blades and has a depth control mechanism. For finer work with density up to 40 follicular units per sq. cm, a 20 or 21 gauge solid or hollow needle is employed.
6. Role of the Surgical Laser
It is clear that the lasers of 2-3 years ago are generally not satisfactory for mega-session work because of potential thermal damage to the remaining skin elements. This can be serious enough to cause large areas of scalp necrosis if grafts are closely spaced.(57, 58) Research is continuing and laser technology is changing so rapidly it is very likely that the new age Erbium lasers will be useful aids in future years. (59, 60)
Complications of Follicular Unit Transplantation
There are no complications specific to the follicular transplantation technique but because of the large number of units involved, there is, with the mega-session technique, a higher probability of some inclusion cysts and graft ischemia occurring.
While some of this increase is due only to the larger numbers, in other cases increased boredom and fatigue in the surgical Assistants is a contributing factor, particularly when the sessions involve more than 2000 closely spaced grafts.
Poor growth.
Poor growth or failure of growth have been much discussed sequelae of mega-sessions in past years. (41) There seems little doubt that much of this may be due to human factors ( termed “H-factor” by Dr Joseph. Greco and will be discussed below. There may be ischaemic elements as well, due to prolonged vasoconstrictor action or the very close spacing of the grafts in some cases.
H-factor
Dr Joseph Greco Jr. first wrote of the human or “H” – factor in hair transplantation in 1994 (61) and enlarged upon this in 1996 (62). Without doubt, human error and carelessness has always been a hazard to hair transplants. Physical damage may be caused by desiccation, forceps pressure or by scalpel slip. Biochemical damage caused by the effect of water, saline, antiseptics, alcohol or hydrogen peroxide.
With the smaller grafts and the use of finer instruments the risk of damage to growth centers is greatly increased. The pressure exerted by a micro-dissector tip may be up to 10 times greater than what it was with the larger graft forceps. (63)
This is analogous with the damaging effects of a 100 pound woman’s stiletto heel on a vinyl floor. Her heel pressure exerted per square cm. of surface, is approximately 10 times greater than that of a 4 ton elephant’s foot. Because of the vast number of follicular cells involved at the growth center of even a single hair, some surgeons doubt if forceps pressure can be a significant factor in growth retardation. Further research is being undertaken into this important subject and Gandelman showed in 1998 that the main damage to grafts did not come from forceps pressure but from desiccation.
He demonstrated that in an air conditioned O.R. at 20 degrees, grafts placed on the dorsum of the gloved hand were irreversibly damaged within 3 minutes. (64)
Donor area scarring.
This can be a problem at times (65) Some patients scar badly after the removal of even a narrow strip. A large session may involve removing a tapered donor strip 25 cm long and 2 cm wide from the occiput. In most cases, this gap closes with ease but may widen in subsequent months. Attempts to correct these scars usually result in only minimal improvement. (66)
Some scar problems occur only after a second wide donor strip is removed. Others may result from taking the strip too low in the donor site. This region seems to be more prone to scar widening and hypertrophy, possibly because of the neck mobility in that region. Attempts to correct or even slightly improve these scars are often exceedingly difficult.
The Dissatisfied Patient

No review of hair replacement techniques would be complete without a discussion of the factors which lead to patient dissatisfaction with their results. The dissatisfaction rate is approximately 2% even in the best clinics. Furthermore, it is apparent to the author that the satisfaction rate with hair transplant procedures has not changed substantially over a period of 30 years although the objective standards have improved enormously in this period. Indeed, as more is now expected of modern technique and total surgical fees increase, patients are more likely to be unhappy and even litigious, if the results fail to meet their heightened expectations. (67)
There are several factors at play here, not the least of which (encouraged by aggressive litigation lawyers) is the rapidly increasing tendency for dissatisfied patients to sue their surgeon. Some doctors aggravate the problem by advertising that results are “undetectable” and “painless” and that “only one session is needed”. Although all these claims may be true for some fortunate individuals, they are by no means the general rule and post-operative pain and lack of graft hair density are common grumbles by patients at follow-up. Some patients are acutely disappointed with their results and angry with the surgeon and this is particularly the case if they have not been carefully counseled before surgery. As Hair Restoration Surgery has become ever more commercial, some physician’s claims have become outrageous and this unfortunate trend may be expected to continue as competition for patients become even more intense.
It must not be forgotten that however careful and ethical the operating surgeon, there is a small group of patients who are very difficult to satisfy. It is unlikely that these individuals would ever be completely happy, even if their results were in the top percentile of excellence, as their expectations are so high and their self-image is so low.
Many of these patients suffer from endogenous depression but this can be notoriously difficult to diagnose in the initial consultation. Sometimes the surgeon can get a clue from the patient’s past history but many patients conceal psychiatric problems during the initial consultation. Thus the surgeon must rely on his intuition and experience to try to identify these difficult individuals and one is bound to be caught occasionally.
The very young and over-anxious patient is an obvious potential problem case but how young and how anxious do they have to be before we exclude them from our operating lists? Some surgeons insist that their patients be 35 or older but most select a figure of somewhere between 22 and 25 as minimum age and are resigned to having a small percentage of dissatisfied patients. (68)
There is also the common presentation of young men with very early hair loss and a psychological reaction out of all proportion to the loss. Experience has shown that young men aged 18-28 have a later dissatisfaction rate which is vastly higher than any other later age group. This is due to a variety of factors that have been discussed at length in the journals and textbooks. (69, 70, 71, ). Chief amongst these is emotional immaturity.
These men will drop out of work or university, withdraw from all social contact, and will sit in the surgeon’s office with a cap pulled firmly around their ears. These men undoubtedly have psychiatric problems and surgery should be firmly rejected or deferred. If a decision is made to proceed it is comforting to have a psychiatrist’s opinion and blessing well before surgery.There is no doubt that the conservative surgeon will have fewer problem patients but then he will also have a lot fewer patients in general, as the 20-35-year-old group makes up at least one-third of the average hair replacement clientele. This high rejection rate would result in a large number of otherwise suitable young men being denied the undoubted benefits which would result from a more luxuriant head of hair.
Finally, but most important of all, is the undoubted fact that not all patients are suitable for surgery. It is imperative that the surgeon ascertains the patient’s wishes and requirements during the initial consultation. If these desires are unrealistic then this must be carefully discussed with the patient. The donor hair varies enormously in both quantity and quality as does the size of the balding area. Add to this the almost inevitable further expansion of the patient’s bald area with time together with a concurrent reduction of potential donor hair and one has an equation which is sure to lead to distress for some men in years to come. The surgeon must be prepared to reject a least 10% of patients seeking hair restoration surgery.
The Future of Hair Transplant Surgery
At the time of writing, the possibilities for further surgical advances seem slim and the way ahead appears to be mostly medical. Better 5 alpha-reductase inhibitors are under trial at present and cloning and gene therapy are being actively discussed.
There are however a few openings for further improvement in the surgical department. Most transplanted hair seems to undergo immediate telogen and 3 months generally elapses before regrowth occurs. If a way was found to bypass this phase long hair could be transplanted with obvious cosmetic benefits to the patient. The topical use of 2% minoxidil before and after surgery has been claimed to increase the percentage of growing hairs but further careful studies are needed on this point. (72)
Mechanical harvesting of grafts and mechanization of the implantation process are both currently under investigation and a number of mechanical devices have already been patented by Crassas, Choi, Boudjema, Rassman, and Markman. Although these do not yet meet with general approval from the profession, further advances in this direction may be expected in the years ahead.( 73,74, 75, 76 , 77, )There is still no general agreement about such fundamentals as the best methods of wound suturing, post-operative wound care or the management of the implanted grafts. All these facets of hair restoration and others need to be subjected to closer scientific scrutiny in the years ahead.
Conclusions
Hair restoration surgery is undoubtedly here to stay, even if the medical prevention of male baldness becomes more commonplace in the future. A mega session with dense packing of follicular units may not be the optimal treatment in every case however and larger units are acceptable to many patients with fair or gray hair. It is not essential that all physicians should equip their offices with the staff and facilities for performing 3000 grafts at a sitting. Sessions of up to 1500 mini grafts or follicular units are safe and within the scope of any small office possessed of at least two capable assistants. If three or four assistants are available then the procedure becomes much less fatiguing. For larger operations, proportionally more staff members are required and the technical difficulties, staff management problems and potential for surgical complications begin to climb exponentially.
Whatever the technique, the benefits of new hair growth resulting from carefully planned and executed hair restoration surgery cannot be denied and the operation is firmly entrenched in the surgical repertoire.
The same 5 hair follicular group appears to consist of two hair and three hair unit.
Follicular groups exist in symmetrical patterns, although there is a somewhat irregular arrangement of the follicular groups within the pattern. Jimenez and Ruifernandez first noted the formula L = k / sq rt of n, where L is the density of hairs in square millimeters, k is a constant depending on the geometric spacing of the follicular units, and n is the density of hair in square centimeters. I have evaluated their formula and found it to be accurate. The geometric arrangement of follicular units follows a triangular pattern. k is 10.7 for a triangular pattern. In this case, the density of follicular units must equal 114.5 per square centimeters for the distance between the follicular units to equal 1 mm. The distance between the follicular units should be measured from the center of the follicular unit.
By Richard Shiell, MD. MODERN HAIR RESTORATION SURGERY
A REVIEW FOR CLINICS OF DERMATOLOGY
By Richard C. Shiell M.B., B.S.
Melbourne, Australia.
Dr. Richard C. Shiell,
Suite 203, 34 Queens Rd.,
Melbourne, Victoria,
Australia, 3004.
Telephone 613-9867-6255
Fax 613-9866-3596